- 1. Chand SP, Arif H. Depression. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-.
- 2. Cui, L., Li, S., Wang, S. et al. Major depressive disorder: hypothesis, mechanism, prevention and treatment. Sig Transduct Target Ther 9, 30 (2024).
- 3. Moret, C., & Briley, M. (2011). The importance of norepinephrine in depression. Neuropsychiatric disease and treatment, 7(Suppl 1), 9–13.
- 4. Diehl, D. J., & Gershon, S. (1992). The role of dopamine in mood disorders. Comprehensive Psychiatry, 33(2), 115–120.
- 5. Pacher, P., & Kecskemeti, V. (2004). Trends in the development of new antidepressants. Current medicinal chemistry, 11(7), 925–943.
- 6. Stachowicz K, Sowa-Kućma M (2022). The treatment of depression — searching for new ideas. Front. Pharmacology. 13:896848. Volume 13 – 2022.
- 7. Hillhouse, T. M., & Porter, J. H. (2015). A brief history of the development of antidepressant drugs. Experimental and Clinical Psychopharmacology, 23(1), 1–21.
- 8. Keller MB, Ryan ND, Strober M, et al. Efficacy of paroxetine in adolescent major depression. J Am Acad Child Adolesc Psychiatry. 2001 Jul;40(7):762-72.
- 9. Pain Management Secrets, 3rd edition. By Andrew Dubin MD MS, Julie Pilitsis MD PhD, Gary McClean MD.
- 10. Oiu HJ, Hong CJ, Chan CH. Paroxetine vs imipramine in Chinese patients. Zhonghua Yi Xue Za Zhi (Taipei). 1996 Jun;57(6):418-23.
- 11. Rapaport MH, Schneider LS, Dunner DL, et al. Controlled-release paroxetine in late-life depression. J Clin Psychiatry. 2003 Sep;64(9):1065-74.
- 12. Yonkers KA, Lin H, Howell HB, et al. Paroxetine in postpartum women. J Clin Psychiatry. 2008 Apr;69(4):659-65.
- 13. https://www.ncbi.nlm.nih.gov/books/NBK538174/
- 14. https://www.researchgate.net/publication/8157458
- 15. https://www.nhs.uk/mental-health/conditions/depression-in-adults/diagnosis
- 16. Gameroff MJ, Wickramaratne P, Weissman MM. SAS-SR short forms. Int J Methods Psychiatr Res. 2012;21(1):52-65.
- 17. Lin S, Carvalho MS, Viana MC. Depression as measure of health-related quality of life. SAGE Open Med. 2016;4:2050312116671725.
- 18. Borong Zhou, Shuangyan Xie, Jiajia Hu, et al. Paroxetine in postmenopausal depression. Guangdong Mental Health Center, China.
- 19. Tharoor H, Vasantha N, Suresh PS. Diagnostic and Statistical Manual of Mental Disorders, 10-ICD: History and Context. AJNR Am J Neuroradiol. 2016 Apr;37(4):596-9.
- 20. Nasreddine, Z.S., et al. Montreal Cognitive Assessment (MoCA): Concept and Clinical Review.
- 21. Lezak M, Howieson D, Loring D. Neuropsychological Assessment. Springer-Verlag.
- 22. Jean Raymond UD. Clinical global impression scale. Innov Clin Neurosci. 2014;11(1-2):93-101.
- 23. Dong-mei DUAN, et al. Paroxetine with Fluvoxetine for Somatic Depression. J Tradit Chin Med. 2009;25(3):167-173.
Efficacy of Paroxetine in Treating
Depression Across
Different Demographics: A Literature Review

Affiliations
Faculty of Medicine Ivabe Javakhishvili Tbilisi State University.
*Corresponding Author: Zainab Sayyed, Faculty of Medicine Ivabe Javakhishvili Tbilisi State University
Citation: Zainab Sayyed. Efficacy of Paroxetine in Treating Depression Across Different Demographics: A Literature Review. Collect J Neurol. Vol 2 (1) 2025; ART0063.

Abstract
This literature review examines the efficacy of
paroxetine, a
Selective Serotonin Reuptake
Inhibitor (SSRI), in treating depression among
adolescents, elderly
patients, postpartum women, and
postmenopausal women. Depression is a prevalent disorder
with
complex etiologies, influenced by
genetic, environmental, and neurobiological factors.
This review
synthesizes findings from multiple
studies to assess the effectiveness of paroxetine in
alleviating
depressive symptoms across these
demographics. Key studies indicate that paroxetine
effectively
reduces depression scores in adolescents
and elderly patients, often outperforming placebo and
showing
comparable or superior results to other
antidepressants, such as imipramine. In adolescents,
paroxetine led
to faster improvement and fewer
severe side effects compared to imipramine. Among
elderly patients,
both immediate-release and
controlled-release formulations significantly improved
depression
scores, although higher dropout
rates due to adverse effects were noted. In postpartum
women,
paroxetine did not significantly
outperform placebo, though certain measures indicated
improvement.
In postmenopausal women,
paroxetine treatment was associated with increased
estrogen levels
and improvements in cognitive
function and anxiety/depression scores, suggesting a
potential link
between hormone levels and
treatment efficacy. Overall, paroxetine demonstrates
substantial
efficacy in treating depression with
a generally favorable safety profile. However,
variations in
response across different populations
and the presence of side effects underscore the need for
personalized treatment approaches. Further
research with diverse populations and long-term
follow-up is
recommended to validate these findings
and refine treatment strategies.
Keywords: Paroxetine, Selective
serotonin reuptake
inhibitor, Imipramine, Estrogen, Cognitive
function, Depression treatment.
Introduction
Depression affects approximately 17 million adults in
the United
States; however, the actual
prevalence is likely higher, as many individuals have
yet to seek
medical help. Among adults aged
60 years and older, depression is three times more
common compared
to those aged 18 to 29 years.
Additionally, adolescent females are 1.5 to 3 times more
likely to
experience depression than their male
counterparts. Major depressive disorder (MDD) has a
complex etiology
influenced by both genetic
and environmental factors [1]. Several hypotheses have
been proposed
to explain the pathogenesis of
MDD, including:
(i) The monoamine hypothesis,
(ii) Dysfunction of the
Hypothalamic-Pituitary-Adrenal (HPA)
axis,
(iii) The inflammation hypothesis,
(iv) Genetic and epigenetic anomalies,
(v) Structural and functional brain remodeling, and
(vi) Social and Psychological factors [2].
Research suggests that late-onset depression is less likely to have a genetic basis compared to early-onset depression. In elderly patients, biological risk factors such as neurodegenerative diseases (e.g., Parkinson’s, Alzheimer’s), stroke, multiple sclerosis, seizure disorders, cancer, macular degeneration, and chronic pain contribute to depression. Additionally, psychological stressors— including the death of a loved one, social isolation, financial difficulties, and interpersonal conflicts— can act as triggers for depressive episodes [1]. The precise pathophysiology of MDD remains unclear. Available data suggest that neurotransmitter availability, receptor modulation, and sensitivity all contribute to emotional symptoms [1]. Preclinical and clinical studies indicate that disturbances in serotonin (5-HT) activity in the central nervous system play a critical role in MDD pathogenesis. Other neurotransmitters implicated in MDD include Norepinephrine (NE), Dopamine (DA), Glutamate, and Brain-Derived Neurotrophic Factor (BDNF) [1]. Serotonin (5-HT) is a crucial neuromodulator with neuroplastic properties. The 5-HT hypothesis suggests that lower serotonin levels increase the risk of depression. Studies have found reduced levels of L-tryptophan (a precursor to serotonin) and serotonin itself in the blood platelets of depressed individuals. Various serotonin receptors—including 5-HT1A, 5-HT1B, 5-HT2A, 5-HT2B, 5-HT2C, 5-HT3, 5-HT4, 5-HT6, and 5-HT7—have been implicated in depression [2]. Norepinephrine (NE) plays a significant role in the development and treatment of depressive disorders. NE signaling from the locus coeruleus to the limbic system, which regulates emotions and cognition, is disrupted in MDD. Postmortem studies have revealed substantial biochemical and functional differences in the NE system between depressed individuals and healthy controls. Pharmacological interventions that reduce NE levels increase the likelihood of relapse in recovered patients, whereas genetic modifications that enhance NE neurotransmission have been shown to protect animals from stress-induced depressive behaviors [3]. Additionally, decreased NE transporter binding has been observed in postmortem brain tissues of individuals with MDD, suggesting a potential pathophysiological mechanism [3]. Dopamine (DA) is also implicated in depression. In experimental models where rats are subjected to unpredictable electric shocks, dopamine levels in subcortical brain regions are significantly reduced. Administration of dopamine antagonists worsens learning deficits in these rats, while dopamine agonists improve cognitive function. These findings highlight dopamine’s role in depression and its potential as a target for therapeutic intervention [4].
Methodology
This study employed a systematic literature review to evaluate the efficacy and safety of paroxetine in treating depression across various demographic groups, including adolescents, elderly patients, postpartum women, and postmenopausal women. The review process followed these key steps:
- Study Selection Criteria – Included research studies with well-defined methodologies, adequate sample sizes, and relevant outcome measures.
- Data Extraction – Focused on study design, participant characteristics, dosage regimens, and adverse effects.
- Comparative Analysis – Evaluated the safety and tolerability profiles of paroxetine in contrast to other antidepressants, particularly imipramine.
- Bias Considerations – Addressed potential biases, including publication bias, to ensure accurate representation of results.
- Referencing and Citation Management – Ensured proper citations throughout the review process.
- Review Structure – Provided a comprehensive overview of methodologies used in the included studies, identifying limitations and offering recommendations for future research.
Background
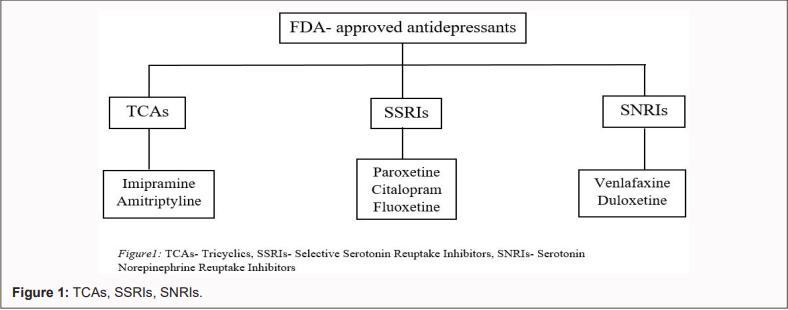
The development of antidepressant medications has evolved significantly since the 1960s and 1970s, with the introduction of Selective Serotonin Reuptake Inhibitors (SSRIs) following earlier advancements in Tricyclic Antidepressants (TCAs) and Monoamine Oxidase Inhibitors (MAOIs) in the mid-1950s [5]. Among the most effective pharmacological treatments for depression are Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs) and SSRIs. However, antidepressant therapy often comes with significant side effects and variable efficacy. Additionally, drug interactions must be considered, particularly in patients with coexisting medical conditions [6]. SSRIs (e.g., paroxetine) Selectively Inhibit Serotonin Reuptake at central synapses. Given that serotonin inactivation occurs primarily through reuptake, blocking the Serotonin Transporter (SERT) leads to increased serotonin availability in the synapses. However, this initial increase activates presynaptic autoreceptors, temporarily reducing serotonin neurotransmission [5]. SSRIs exhibit significantly higher selectivity for serotonin reuptake inhibition than norepinephrine, with a selectivity ratio ranging from 20 to 1500 times. Moreover, SSRIs display minimal binding affinity for Dopamine D2, Histamine H1, Muscarinic, and Adrenergic α1, α2, and β Receptors. Unlike Tricyclic Antidepressants (TCAs), SSRIs—such as Citalopram and Fluoxetine—exert little to no direct pharmacological effect on Postsynaptic Serotonin Receptors (5-HT1A, 5-HT2A, 5-HT2C) and do not promote specific serotonin or norepinephrine release [7]. In contrast, SNRIs (e.g., venlafaxine) block both serotonin and norepinephrine reuptake at their respective transporters. Unlike TCAs, SNRIs exhibit negligible to no activity at Histamine (H1), Muscarinic, Adrenergic (A1, A2, B), and Dopamine Receptors [7]. Meanwhile, TCAs (e.g., imipramine) influence multiple pharmacological targets, including:
- Inhibition of norepinephrine and serotonin reuptake transporters,
- Blockade of postsynaptic muscarinic, histamine H1, and adrenergic α1 and α2 receptors [7].
This review provides an in-depth evaluation of antidepressant benefits and limitations, emphasizing the need for precise and personalized treatment approaches in managing depression.
Body
Paroxetine in the treatment of adolescent major depression: M.B Keller, N.D Ryan, M Strober, et al. [8] performed a study for at least 8-week duration on adolescents with major depression by comparing paroxetine with placebo and imipramine with placebo. The trial was focused in the US (10 centers) and in Canada (2 centers), where screening for eligibility was done on 425 individuals, and 275 individuals were assigned to experimental treatment randomly. Individuals fulfilling the DSM-IV criteria for major depression ranged in age from 12 to 18 years. DSM-IV (Diagnostic and Statistical Manual of Mental Disorders) of the American Psychiatric Association is an official manual that provides a framework for classifying and defining disorders and their diagnostic criteria [8,9]. Clinical interviews were held to confirm the diagnosis by utilizing Affected Disorders and Schizophrenia for Adolescent - Lifetime Version (KSADS-L). Criteria included HAM-D (also known as HRS-D17 scale; has 17 items referring to depressive symptoms from the past week [8,13]). HAM-D scoring for the HRS-D17 version: score 10–13 is mild, 14–17 is mild to moderate, and >17 indicates moderate to severe depression [8,14]. Other criteria included a minimum HAM-D score of 12, Children’s Global Assessment Scale score < 60, and a score of at least 80 on the Peabody Picture Vocabulary Test. Exclusion criteria involved individuals with various current or lifetime DSM-IV diagnoses (e.g., bipolar disorder, schizoaffective disorders), PTSD within 12 months of recruitment, substance use, recent antidepressant use, and females who were pregnant or breastfeeding. Screening began with telephone assessments followed by on-site evaluations [8]. A 7–14 day screening period without placebo assessed the severity and persistence of symptoms. Physical exams and lab work were also conducted. Qualified individuals were randomly treated in a 1:1:1 ratio with paroxetine, imipramine, or placebo for 8 weeks. Paroxetine was administered at 20 mg in the morning for 4 weeks, increasing to 30 mg in week 5 and to 40 mg by week 6–8 if necessary. Imipramine was initiated at 50 mg/day, increased to 200 mg by week 4, 250 mg by week 5, and 300 mg by weeks 6–8, if necessary. Doses ≥100 mg were split between morning and evening. During weeks 1–2, participants received one active drug in the morning and a placebo in the evening. Placebo group participants received two placebo capsules daily. By week 3, participants received one active and two active or placebo capsules in morning and evening, respectively. Week 4 dosage included one active drug, a placebo capsule in the morning, and two active drugs in the evening. Week 5 dosage mirrored week 4 or was titrated to 5 or 6 capsules total. Participants completing the trial could continue the treatment for 6 additional months. Dropouts tapered off the treatment over 7–17 days [8]. Another similar study was conducted by Chiu HJ, Hong CJ, Chan CH et al. [10] in 1994 on Chinese patients with depressive disorders. HAM-D, CGI, and adverse effects were assessed using TESS (Treatment Emergent Symptoms Scale). The CGI scale provides a clinician's global view on the patient's functioning pre- and post-treatment. It consists of: 1) a severity assessment on a 1–7 scale, and 2) a 7-point scale measuring treatment-related changes [10,21]. TESS evaluates adverse symptoms during treatment, including their severity and relation to the medication. Scores: 0 = no symptoms; 2 = mild; 3 = moderate (functional impact); 4 = severe (significant life impact) [10,22]. Patients with HAM-D scores ≥18 were treated with paroxetine (20–30 mg daily) or imipramine (100–125 mg daily) for 6 weeks. Among 40 patients, 5 withdrew due to adverse effects related to impatience, leaving 35 participants for analysis [10].
Controlled-release paroxetine in the treatment of late-life depression: Rapaport MH, Schneider LS, Dunner DL, et al. conducted a multicenter, placebo-controlled, double-blind, randomized 12-week trial involving 319 elderly Americans (mean age = 70 years) to evaluate paroxetine's efficacy in treating Major Depressive Disorder (MDD). Participants received either controlled-release paroxetine (50 mg/day, N = 104), immediate-release paroxetine (40 mg/day, N = 106), or placebo (N = 109). Inclusion criteria required a diagnosis of MDD according to DSM-IV and a HAM-D score of ≥18 on the 17-item scale [11].
Postpartum depression: Yonkers KA, Lin H, Howell HB, et al. conducted a multicenter, parallel, placebo-controlled trial between 1997 and 2004 (before mandatory clinical trial registration) to assess paroxetine's effectiveness in treating acute postpartum major depressive disorder. Seventy women were enrolled and randomly assigned to treatment over an 8-week period, although only 31 completed the trial. Study sites included Yale University School of Medicine/Bridgeport Hospital, University of Texas Southwestern Medical Center, and Massachusetts General Hospital. Eligibility criteria for the study included: minimum age of 16 years and onset of MDD within three months postpartum. Depression severity was evaluated using the 17-item Hamilton Rating Scale for Depression (HRS-D17), with a required score of at least 16 out of 17 breastfeeding women were also included in the study. Exclusion criteria were: alcohol or drug abuse within the past 6 months, evidence of current psychotic symptoms, current pharmacotherapy or psychotherapy for a psychiatric disorder, current pregnancy, suicidal ideation, unwillingness to participate, or onset of MDD prior to delivery [12]. Participants underwent initial screening by phone or in person to assess eligibility. Eligible women completed a baseline assessment, which included the Structured Clinical Interview for DSM-IV (SCID) for psychiatric diagnosis, Hamilton Rating Scale for Depression (HRS-D17) to assess depression severity, Clinical Global Impression (CGI) severity scale for global clinical evaluation, Inventory of Depression Symptomatology (IDS-SR), and Social Adjustment Scale to evaluate functioning and social adjustment [12,15,16]. The SF-36 Health Status Survey measured eight health dimensions: Physical Functioning (PF), Role Physical (RP), Bodily Pain (BP), General Health (GH), Vitality (VT), Social Functioning (SF), Role Emotional (RE), and Mental Health (MH) [12,17]. Blood and urine tests were also conducted to rule out medical or pregnancy-related exclusion factors. Follow-up assessments occurred weekly from week 1 to week 8 (±7 days) post-randomization, with repeated measures on HRS-D, IDS-SR, and CGI conducted blindly at each visit [12]. Participants were randomly assigned to receive paroxetine or placebo capsules, identical in appearance. A computer-generated randomization schedule (in blocks of four and stratified by site) was used to assign treatments. Initially, participants received 10 mg of paroxetine or placebo daily for weeks 1 and 2. The dose increased to 20 mg daily for weeks 3 and 4 if side effects were tolerable. If less than 30% improvement from baseline was observed, dosage could be further increased to 30 mg at week 4 and up to 40 mg by week 6. Compliance was monitored through pill counts. Participants taking fewer than 80% of the prescribed capsules were considered non-compliant and received appropriate consultation [12].
Post-menopausal woman
The study was performed by Borong Zhou, Shuangyan Xie, Jiajia Hu, et al. [18] between 2011 to 2012, a total of 88 postmenopausal women with depression and anxiety, among which 82 participants completed all the sessions after losing 6 patients to follow-up. According to Stages of Reproductive Aging Workshop criteria women experiencing their last menstrual period ≥ 12 months are considered postmenopausal, and there in this study all the participants were eligible. ICD-10, International Classification of Disease system tracks diseases within a population, [18,19] system was met for standard diagnosis of anxiety and depression. It was made sure that the participants had not taken any psychoactive drugs or hormonal therapies for at least 6 months before and had not had any mood or behavioral diseases before perimenopause. There were 2 groups created and participants were assigned randomly; an experimental group (group- E having 44 cases)- participants in this group were treated with paroxetine, and the other group was the control group (group- C, having 38 cases)- participants in this group were treated with Oryzanol (lipid from rice bran oil- RBO; anti-oxidant and lowers cholesterol). Participant’s anxiety, depression and cognition were kept in check with the help of HAM-A (Hamilton Anxiety Scale), HAM-D (Hamilton Depression Scale), and MoCA-CV (a paper-and-pencil screening instrument for detection of Mild Cognitive Imperilment including- memory, language, attention, concentration, executive functions, visuospatial skills, abstraction, calculation and orientation) assessments prior to measurement of sex hormone; these assessments were done pre- and post- treatment [18,20].
Group- E was given a daily dose of 10 mg paroxetine for the 1st week along with a daily dose of 20 mg for the remaining 6 months. Group- C, for 6 months received 20 mg oryzanol three times a day. Apart from these medications a daily dose of 0.8mg of Alprazolam (class- benzodiazepines; for anxiety, panic disorders and types of seizures) was given to both the groups but later on it was tapered and then stopped [18]. Neuropsychological scale assessment on the participants was done on the basis of the diagnostic criteria of ICD-10 for diagnosing anxiety and depression. The criteria included: 1) HAM-A score ≥ 14 and HAM-D score ≥ 17, this indicates significant anxiety and depression symptoms respectively; 2) encountering major anxiety symptoms for at least 3 months or depression symptoms for at least 2 months. 3) unable to function properly at work and home. Among these participants 39 were diagnosed with mixed anxiety and MDD, 28 of them with anxiety alone, and the rest 15 of them with depression alone. The MoCA-CV scale was used to assess cognitive function. Sex hormones (serum LH, FSH, progesterone, and estrogen) evaluation was done by ELISA kit. Collection of blood samples done after overnight fasting, between 7 am and 8 am, from the cubital vein [18].
Result
In the study done by M. B Keller, N.D Ryan, M Strober, et al. the groups treated had shown significant improvement with paroxetine in comparison with imipramine and placebo for several depression-related disorders in adolescents. The scores used to measure the response rate, mood scales, etc. A high percentage of individuals treated with paroxetine achieved a HAM-D score ≤8. Paroxetine was faster in time course analysis than imipramine and placebo. It also showed to improve depressed mood better than imipramine, which showed no effect on mood at all [8]
Similar study as above done by [10] in 35 Chinese patients with depressive disorders, among which 60% (12/18) were treated with paroxetine and 65% (11/17) were treated with imipramine showed 50% or more reduction in their HAM-D scores. Paroxetine affected their mood positively making it recover to near-normal in the paroxetine group (66.7%) when compared to the imipramine assigned group of patients (35.3%). The difference was not that significant and mean reduction of HAM-D by the end of the trail was also similar between the groups. Along with that, the paroxetine group experienced fewer anticholinergic adverse effects, without any reduction in the efficacy, when compared to imipramine. However, with reduced sample size, and reduced duration and follow-up did affect the overall impact of the study [10]. Rapaport MH, Schneider LS, Dunner DL, et al. performed a study on paroxetine efficacy in late-life MDD. Paroxetine CR and Paroxetine IR showed significant improvement when compared to placebo group on the basis of the HAM-D scale at week 12, with paroxetine CR having marginally better score than paroxetine IR. HAM-D score appeared to be constantly lower for both of the groups when compared to placebo group, HAM-D score for paroxetine CR was 10.0 ± 7.41 and paroxetine IR 10.0 ± 7.10, insignificant difference. Furthermore, a higher proportion of patients treated with paroxetine CR achieved both response (72%) and remission (43%), which shows statistically significant difference when compared to that of placebo group. Paroxetine IR demonstrated quite similar response (65%) and remission (44%) rates, but with lower statistical significance. Particularly, post hoc analysis disclosed the efficacy of paroxetine in patients with both short-term and chronic depression, proposing its significance. Overall, the result of the study concludes efficacy of paroxetine in managing depression (paroxetine CR > paroxetine IR in efficacy) is potent. Nonetheless, due to adverse effects during the treatment, dropout rates in paroxetine CR (12.5%), placebo IR (12.0%), were slightly elevated when compared with placebo (8.3%) group [11]. In study performed by Yonkers KA, Lin H, Howell HB, et al. it was found that paroxetine did not significantly outperform placebo in treating women with post-partum MDD but still had greater improvement in certain measures. Pill count results showed that among the women who were given paroxetine, at one visit 7 (28%) resulted to be non-compliant and at two visits 4 (16%) resulted to be non-compliant. Participants who were assigned for the placebo treatment, at one visit there were 10 (40%) non-compliant, at two visits 3 (12%) were non-compliant, and on four visits only one was non-compliant [12]. Borong Zhou, Shuangyan Xie, Jiajia Hu, et al. performed study on post-menopausal women and effect of paroxetine, which proved that paroxetine significantly increased serum estrogen level in just 6 months of receiving it, in comparison to the control group. Significant drop in serum LH (from 24.18 ± 6.25 MIU/ml to 18.43 ± 4.55 MIU/ml) and FSH (from 50.56 ± 16.78 MIU/ml to 28.90 ± 11.34 MIU/ml) was also noted. With the increase of estrogen levels there was significant raise in MoCA-CV score to 26.92 ± 1.92 from 24.08 ± 2.22 and significant drop in HAM-A and HAM-D scores by paroxetine, in comparison to the control group where HAM-A score decreased, HAM-D and MoCA-CV scores did not change. This happened so as estrogen level is associated to HAM-A, HAM-D, and MoCA-CV pre-treatment and post-treatment with paroxetine. In addition to paroxetine therapy, estradiol (E2) shows positive correlation with MoCA-CV which means that with high level of estrogen cognitive functions are better. Conclusion being estrogen has consistent impact on the neuropsychological scores before and after paroxetine therapy. This study provided us with the relation of estrogen and paroxetine treatment but did not focus enough on the other factors/confounders that could affect the estrogen levels, such as, lifestyle, socioeconomic status, or other medications. Along with the factors affecting estrogen levels, the sample size was also limited, it would have been better with a diverse population to confirm the study. The study also seemed to be focused on the short-term changes in the estrogen level and the effect it has on neuropsychological scores, whereas long-term follow-up could have provided effects on the long run [18].
Safety
Paroxetine was generally well tolerated in the adolescent population, with the majority of side effects being mild to moderate and easily controlled with dosage reduction. These manageable side effects allowed most participants to continue using the medication without significant issues. On the other hand, imipramine resulted in more severe adverse effects, including aberrant ECG readings, prolonged QT intervals, arrhythmias, and postural hypotension. These serious side effects led to over one-third of the participants discontinuing imipramine therapy. Furthermore, there was a notable distinction in the safety and tolerability profiles of the two drugs, as anticholinergic side effects—such as dry mouth, blurred vision, constipation, and urinary retention—were recorded more frequently in the imipramine group than in the paroxetine group. This highlights the greater overall tolerability of paroxetine compared to imipramine in adolescents, making it a more favorable option for this population [10].
Discussion
The reviewed studies on paroxetine in the treatment of depression present several limitations that affect the generalizability and robustness of their findings. One study’s participant population was predominantly from the US and Canada, and the second study was predominantly in the Chinese patients, limiting the applicability of its results to broader, more diverse demographic and cultural backgrounds. Generally, the studies had relatively short durations, ranging from 8 to 12 weeks, which is insufficient for capturing the long-term efficacy and safety of paroxetine in treating major depressive disorder, a condition that often requires prolonged treatment. The impact of the studies is further compromised by reduced sample sizes, incomplete dropout information, and high dropout rates, which undermine the reliability of the findings. Additionally, there was a lack of variety in the racial and ethnic backgrounds of participants, and crucial subgroups, such as individuals with comorbid medical conditions or cognitive impairments, were not sufficiently examined. Moreover, the studies did not adequately address the reasons behind non-compliance among participants, nor did they explore the impact of breastfeeding on treatment outcomes. The absence of direct comparative analysis between different formulations of paroxetine (CR vs. IR) further limits the comprehensive understanding of its efficacy. Future research should aim to include more diverse populations, extend follow-up periods, and provide detailed analyses of compliance factors and subgroup responses to ensure more comprehensive and generalizable results.
Conclusion
The literature review indicates that paroxetine is an effective treatment for Major Depressive Disorder (MDD) across various demographic groups, including adolescents, the elderly, postpartum women, and postmenopausal women. Studies consistently show that paroxetine improves depression symptoms significantly more than placebos and often more than imipramine, with a favorable safety and tolerability profile. However, its efficacy in postpartum depression was less conclusive, and the impact of estrogen levels on treatment outcomes in postmenopausal women requires further research. Overall, paroxetine is well-tolerated and effective, but additional studies focusing on long-term effects and broader populations are recommended to validate these findings.